Predictive Story Mapping for Progressive Memory Loss Patients
The 15-Year Window Nobody Is Using
Alzheimer's progresses across a 15-year timeline from earliest detectable deficits to severe AD, with the clinically diagnosed window averaging 4-8 years of survival post-diagnosis. 7 million Americans currently live with Alzheimer's, a number projected to reach 13 million by 2050. Most of them will die having never been asked to narrate their own lives in structured form.
The opportunity is bracketed by biology. Cognitive decline across 12-24 months reliably predicts future dementia, and biomarker signatures show hazard ratios of 15.1 for MCI-to-dementia conversion. Families now receive warning years before severe decline. They also experience anticipatory grief tied to MCI progression, which motivates them to capture memories while the person they love is still accessible.
What is missing is infrastructure. A daughter who suspects her father has early MCI does not know how to start a structured story capture. She Googles, finds an obituary template, and closes the tab. Twelve months later, her father can no longer recall his first job. Advocacy organizations recommend capturing stories quickly while long-term memories are intact, but recommendations without workflows do not get acted on. Funeral homes that partner with memory-care and MCI clinics can provide the workflow — if they build predictive story mapping as a pre-death service, not a bereavement service.
The business model implications are significant for funeral homes that recognize them. A dementia patient diagnosed at age 72 with a 6-year decline trajectory represents a 72-month customer relationship window, most of which happens before any traditional memorial activity. Funeral homes that treat the 60-month window as a waiting room miss 60 months of value creation. Homes that treat it as a staged capture opportunity build long-arc relationships with families — and simultaneously build tapestries that make the eventual memorial dramatically richer than one assembled in a seven-day post-death window.
Predictive Mapping as Tapestry Forecasting
StoryTapestry's predictive model treats each diagnosed or suspected MCI patient as a tapestry-in-progress. The system maps the known life timeline across seven domains: childhood, education, career, relationships, parenting, community, identity markers. For each domain, it forecasts which threads will be lost first based on cognitive-progression patterns — procedural memory persists longest, episodic memory degrades first, semantic memory sits between.
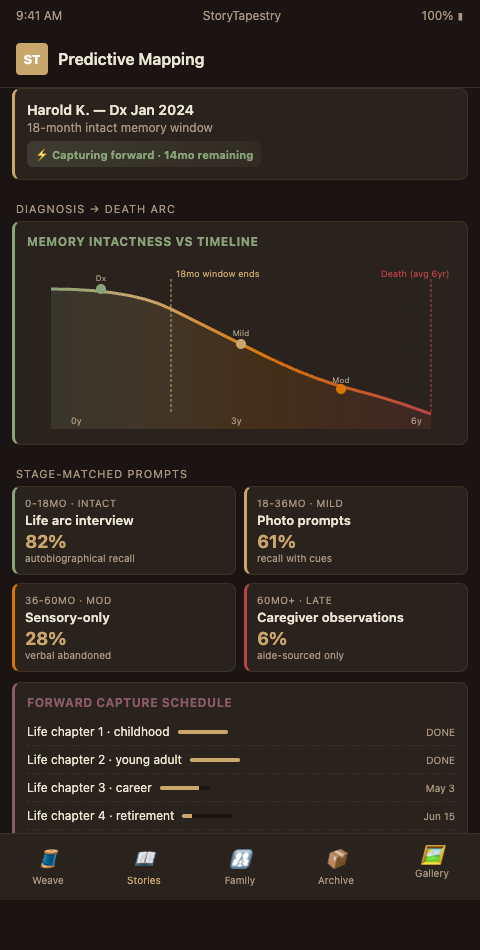
The forecast produces a capture priority. A 68-year-old with MCI whose career was his primary identity marker gets career-domain prompts first, because work narratives are among the earliest to lose specificity. A 74-year-old whose childhood rural farm is the spine of her self-concept gets childhood prompts first, because those deep-past memories, while durable, require specific sensory cues (smells, weather, farm animal names) that family informants cannot reproduce after decline. The mapping is cognitive-stage sensitive, drawing on progression research to sequence interviews.
Threads get woven forward. At diagnosis, the family begins a tapestry. Over 24 months, prompts cycle through priority domains. At month six, the system shifts away from complex narrative prompts toward simpler sensory and recognition prompts as cognition changes. At month 18, the focus shifts to caregiver fragments — spouses, adult children, close friends — who now hold the memories the patient can no longer articulate. By month 36, the tapestry is largely woven from external threads, with the patient's early-captured voice sitting as the central motif.
This is where StoryTapestry differs structurally from obituary-only tools. Traditional memorial software captures after death. Predictive story mapping captures across decline, with the tapestry as a living artifact that families can visit, extend, and use for reminiscence therapy long before the memorial. Nursing homes that run life-story interventions for reminiscence already show this pattern — the artifact is therapeutic, not posthumous.
Capture infrastructure must respect ethical memorial consent boundaries throughout the decline. A patient who consents at month two may no longer have capacity by month 30. StoryTapestry's consent ladder establishes proxy decision-making with the family early, documents the patient's content preferences while capacity remains, and flags any fragment captured after capacity loss for proxy review. This is not a feature — it is a compliance requirement that distinguishes clinically defensible predictive mapping from exploitative data collection.
Funeral home partnerships with MCI clinics, memory-care facilities, and neurologist practices are the delivery channel. A clinic that screens for MCI can offer newly diagnosed families a referral to a "life-story planning session" at the partnered funeral home, framed as advance memorial planning. Families arrive at diagnosis already knowing who will help them capture the narrative. The funeral home gets the relationship at month zero instead of month 60. For passive capture during severe decline, ambient story capture tools complement the predictive-mapping approach by collecting fragments from daily life without demanding active participation.
The tapestry grows through overlapping capture modes. Early-stage captures are primarily first-person: the patient narrates, the funeral home's trained interviewer records, StoryTapestry transcribes and structures. Mid-stage captures shift toward co-narration: the patient contributes what they can, while a spouse or adult child fills in details in real time during sessions. Late-stage captures become primarily third-person: caregivers, family, and community contribute, and ambient capture threads in the patient's own spontaneous utterances. Each capture mode produces different thread types, and the tapestry is structurally richer for containing all three.
Advanced Forecasting Techniques
Stratify patients by decline trajectory, not diagnosis date. Two patients with the same MCI diagnosis can have wildly different 5-year outcomes depending on biomarker profile, comorbidities, and cognitive reserve. StoryTapestry's triage asks the neurologist or memory-care social worker to categorize progression risk as slow, moderate, or rapid. Rapid-progression patients get compressed capture schedules — four domains in the first 90 days rather than 24 months — because their cognitive window may close in under two years.
Use identity anchors to sequence the capture, drawing on biomarker hazard evidence to prioritize the domains most likely to fade first. Ask the family one question at intake: "If this person could tell one story about themselves to their great-grandchildren, what would it be?" The answer reveals the identity anchor. Capture that anchor first, in highest fidelity, because it is the thread the whole tapestry will be organized around. Anchors change as decline progresses; revisit the question every six months during early stages, because the patient's own sense of identity will reorganize as episodic memory fades and semantic memory holds.
Pair predictive mapping with caregiver fragment collection from day one. A common failure mode is waiting until the patient can no longer contribute before bringing caregivers in. By then, caregivers have lost their own context for what the patient remembered. Bring in spouses, adult children, and close friends at month three — while they can still correlate their memories with the patient's active narration. This creates redundancy in the tapestry and lets you reconcile contradictions while the primary source is still arbitrating them.
Integrate with adjacent memorial traditions. Parallel workflows exist for therapeutic memorialization in other contexts, and the predictive-mapping logic transfers where a family faces anticipated loss. In dementia, the loss is slow; in other contexts, it can be sudden. The common structural insight is that memorial work can begin before death, and the family benefits from the process as much as the eventual artifact.
Offer tapestry-review sessions as anticipatory-grief support. Families reviewing the in-progress tapestry at months six, 12, and 24 engage with it as therapy, not only as documentation. Some funeral homes now bill these sessions as bereavement-adjacent services. The revenue stream is smaller than at-need memorial services but the relationship depth is higher, and it produces strong downstream conversion when death occurs.
Coordinate with MCI clinic care plans. Neurologists and geriatric psychiatrists increasingly embed life-story capture in care-plan documentation because reminiscence-adjacent activities have clinical benefit. A funeral home whose predictive mapping output integrates with the patient's care plan becomes a clinical partner, not an outside vendor. This changes how neurologists talk about the service during diagnosis conversations — from "you might want to consider pre-planning" to "this is part of how we manage progression." The referral friction drops dramatically.
Plan for caregiver turnover during long captures. In a 60-month capture, the primary family caregiver may change — a spouse may become ill, an adult child may relocate, a paid caregiver may leave the family's employ. StoryTapestry's caregiver-handoff protocol documents what the outgoing caregiver knew, what they contributed, and how the incoming caregiver can extend the work rather than restart it. Homes that do not plan for this lose continuity at month 24 or 36, usually at the most cognitively thin point in the decline.
Start Your Predictive Mapping Partnership
Every MCI diagnosis in your service area is a family asking "how do we do this." Funeral homes that answer that question with infrastructure, not brochures, become the trusted partner for the full decline and the memorial that follows. StoryTapestry's predictive-mapping module deploys in 60 days, including MCI-clinic outreach templates and neurologist referral workflows tuned for your region's clinical community, with anticipatory-grief research informing how we frame family-facing messaging. Request a partnership kit and we will include a forecasting demo run against a sample patient profile so you can see the tapestry grow forward before you commit to deploying the infrastructure across your practice. The kit arrives within three business days and contains clinic-facing one-pagers, a referral-script template tested with 14 neurology practices, a consent and HIPAA addendum aligned with memory-care hospice partnerships, and sample five-year milestone workflows for three common MCI trajectories.
Partnership onboarding pairs your director with a dedicated mapping specialist who handles clinic outreach in the first 30 days, a platform trainer who certifies two staff on forecasting workflows, and a pricing consultant who builds the pre-need ladder for families at diagnosis, two years in, and late-stage. Funeral homes that deploy the full module typically onboard their first three MCI-referred families inside 90 days and reach 15 active forecasts by month six. Request the partnership kit today and we will schedule the demo within the same week.