When the Storyteller Can't Remember: Ethical Memorial Assembly
The Ethical Weight of Post-Capacity Memorial Assembly
Dementia creates a distinctive ethical situation for memorial assembly that other causes of death do not. When the storyteller has lost the capacity to remember their own preferences, memorial creation for someone in this state raises issues of representing a person through posthumous storytelling that demand frameworks protecting both autonomy and dignity. Decision-making capacity is frequently compromised even in moderate dementia, and by the severe stages the patient cannot participate in any meaningful planning of their own memorial (PMC - Dementia Decision-Making Capacity). When family members try to speak for the deceased, they face a bioethical puzzle: whose preferences are they actually honoring, and how much interpretive latitude is ethically appropriate? Capacity evaluation research confirms that surrogate decision-making in dementia contexts requires structured frameworks, not improvisation (BMC Medical Ethics - Capacity Evaluation).
The AMA Journal of Ethics argues that autonomous decisions made by a person reflect their continuous self, and that surrogate decisions made after capacity loss should honor the prior autonomous self rather than substitute new preferences (AMA Journal of Ethics - Dementia QoL). For memorial assembly, this translates into an ethical standard that funeral directors partnering with memory care facilities must navigate with every case: represent who the person was while autonomous, acknowledge the reality of who they became during decline, and do neither at the expense of the other. Without a deliberate framework, directors default to whichever family member is most assertive, which is ethically thin.
Weaving an Ethical Framework Into the Memorial Tapestry
StoryTapestry builds post-capacity memorial assembly on three ethical principles that structure the platform's consent and representation workflows. The tapestry metaphor is not decorative here; it reflects the underlying ethical claim that a life contains both the pre-disease person and the decline-era person, and a memorial tapestry woven faithfully must include threads from both eras without letting either dominate or erase the other. Personhood research in dementia bioethics argues explicitly that the patient remains a continuous person throughout the disease, even as their capacities change (PMC - Personhood Dementia Bioethics).
The first principle is documented preferences first. Advance directives, informal expressions captured in writing, and pre-decline recorded statements are the strongest evidence of what the deceased would have wanted. Alzheimer's Association guidance on legal documents confirms that advance directives provide the surrogate framework for post-capacity decisions (Alzheimer's Association - Legal Documents and Decision Making). StoryTapestry prompts families during intake to identify any documented memorial preferences and weighs those explicitly in the assembly workflow. If the deceased said in a 2015 conversation with her daughter that she did not want a religious service, that preference takes precedence over a 2025 sibling's different preference, regardless of how articulately the sibling argues.
The second principle is consistent-character representation. When documented preferences are absent, surrogate decisions should honor the character the deceased consistently demonstrated while autonomous. Research on informed consent in Alzheimer research emphasizes that surrogate decision-making requires attention to substituted judgment, not best-interests substitution (PMC - Informed Consent Alzheimer Research). A woman who privately treasured classical music but publicly attended hymn-filled services all her life has two consistent characters; StoryTapestry surfaces this tension during intake rather than letting family members project their own preferences.
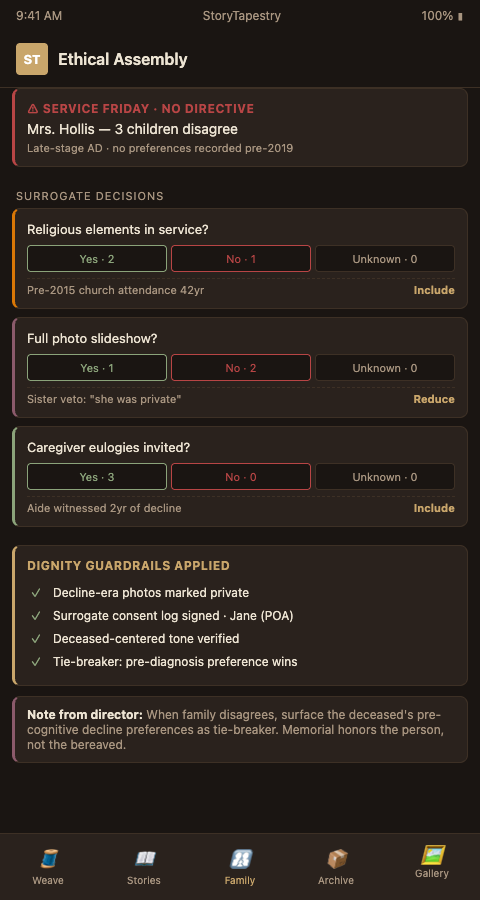
The third principle is proportional decline representation. The person's dementia years were real, and erasing them in the memorial is its own form of dishonesty. But defining the person entirely by their decline is the opposite dishonesty. StoryTapestry structures the final memorial with explicit era-weighting that families review: what fraction of the tribute represents the pre-diagnosis person, what fraction represents the decline era as witnessed by caregivers, and how the two interact. This is exactly the kind of framework the cognitive decline grief research suggests families need but rarely receive from funeral homes without specific memory care training. Combined with sensitive interview training, it produces memorials that pass the ethical test families carry with them after the service.
The three principles interact in practice, and the interaction is often where directors without a framework make errors that haunt families afterward. A documented pre-decline preference against religious elements, a consistently demonstrated character that participated in a faith community, and a decline-era pattern of responding to hymn recordings at the memory care facility produce apparent contradictions that can only be resolved by talking through them explicitly with the family. StoryTapestry surfaces the contradictions during intake rather than letting them silently resolve toward whichever family member speaks loudest, and the structured conversation that follows produces memorials families describe as having honored the person's full complexity rather than flattening her to a single dimension. The director's role becomes guide through ethical terrain the family cannot navigate alone, and this is a distinctly different service than the arrangement-coordinator role that default funeral workflows assume.
Advanced Ethical Tactics for Dementia Memorial Assembly
Three advanced tactics help memory care funeral homes handle the hardest ethical situations. First, require two-signature consent when surrogate decisions override pre-decline documented preferences. If the deceased specified in a 2017 letter that she wanted cremation and three adult children now request full traditional burial, StoryTapestry flags the contradiction and requires explicit documentation of why the surrogate decision differs. This creates an audit trail that protects the funeral home ethically and often surfaces family conflict that would otherwise erupt after the service.
Second, apply privacy consent protocols from the perinatal bereavement context to dementia contexts. Perinatal memorial programs have rigorous consent frameworks because infants cannot consent to their own memorial. The structural parallel to late-stage dementia patients is close, and the ethical infrastructure transfers well. Both contexts involve memorial subjects who cannot participate in their own representation, both involve grieving surrogates who may project their own needs onto representational decisions, and both require professional mediation.
Third, include the deceased's own voice wherever it exists. Recordings from pre-decline years, written letters, journal entries, and quoted statements from family members become first-person threads in the memorial tapestry. When the patient's actual voice is present in the service, the ethical burden of surrogate representation decreases proportionally. This is why pre-decline gathering produces memorials that feel ethically grounded in ways that purely posthumous assembly cannot match.
Fourth, treat sibling disagreement as information rather than friction to be minimized. When three adult children cannot agree on whether their mother would have wanted a religious service, the disagreement itself usually indicates that the mother demonstrated different sides of herself to different children and none of them has the complete picture alone. StoryTapestry's sibling attribution structure captures each child's evidence as a distinct thread rather than forcing a consensus narrative, and the memorial reflects the actual plurality of the mother's self-presentation across her relationships. The funeral director who facilitates this well often hears siblings say after the service that they finally understood a part of their mother they had missed, which is a bereavement outcome that forced-consensus memorials cannot produce.
Fifth, document the ethical reasoning itself in the family's archive. When a difficult decision is made (honor the 2015 documented preference over the 2025 family request, include the decline-era photos over family objection, weight pre-diagnosis at 60% of tribute time over the caregiver's preferred 40%), the reasoning should be written down and preserved with the memorial archive. Years later, adult children or grandchildren who ask why the service unfolded as it did can see the reasoning rather than wondering if they were overruled or ignored. This transparency is its own form of ethical rigor, and families who discover the decision log during later grief processing describe it as clarifying rather than controlling.
Bring Ethical Rigor to Your Memory Care Memorial Services
Funeral homes without an ethical framework for post-capacity memorial assembly produce tributes that haunt families with questions about whether they honored the deceased faithfully. Funeral homes with a framework deliver memorials that families describe as ethically settled, even when the dementia journey was ambiguous. StoryTapestry provides the consent hierarchy structures, surrogate attestation workflows, and era-weighting tools that make ethical assembly operational rather than aspirational. Contact StoryTapestry to discuss how memory care funeral homes can integrate bioethical rigor into every memorial they assemble for families whose loved ones could no longer speak for themselves.
Pilot funeral homes receive direct product team support to implement the three-principle ethical framework in their arrangement conference workflow, train directors on the two-signature consent protocol for surrogate overrides of documented preferences, and establish the era-weighting review process that produces proportional decline representation. Your first ten post-capacity memorial assemblies on the platform receive concierge support including bioethicist review of the hardest cases (unclear documented preferences, irreconcilable sibling disagreement, late-discovered advance directives) so your directors learn the reasoning patterns that apply to future cases. Your feedback shapes the production release of the consent hierarchy structures, the sibling attribution architecture, the documented-reasoning archive, and the voice-of-the-deceased inclusion tools that reduce surrogate ethical burden by elevating first-person threads when they exist.
Schedule a consultation to discuss how your firm can make bioethical rigor a standard capability across every memorial you assemble for dementia families whose loved ones could no longer speak for themselves during planning.