How to Preserve Pre-Diagnosis Memories Alongside Caregiver Accounts
The Pre-Diagnosis Memory Window Most Families Miss
Autobiographical memory degrades on a predictable trajectory in Alzheimer's disease, with semantic memory (facts about one's life) persisting longer than episodic memory (specific events) but both eventually compromised (Frontiers - Autobiographical Memory in Alzheimer's Review). Families typically discover the importance of story capture only after diagnosis, when the most vivid narrative material is already becoming inaccessible. Systematic review evidence confirms that autobiographical memory impairment directly degrades self-awareness and identity as dementia progresses (PMC - Autobiographical Memory AD Systematic Review).
The pre-diagnosis window is actually longer than most families realize. Mild cognitive impairment (MCI) precedes Alzheimer's diagnosis by an average of 3 to 7 years, and anticipatory grief research shows that caregivers experience meaningful loss during MCI and early dementia stages (PMC - Anticipatory Grief Caregivers Dementia). Yet funeral homes partnering with memory care facilities consistently encounter families who did not start gathering stories until moderate-stage dementia, when the patient can no longer narrate their own life with reliable detail. The gap between when families could have captured pre-diagnosis memories and when they actually try is typically four to seven years of irretrievable material.
Weaving Pre-Diagnosis and Caregiver-Era Threads Together
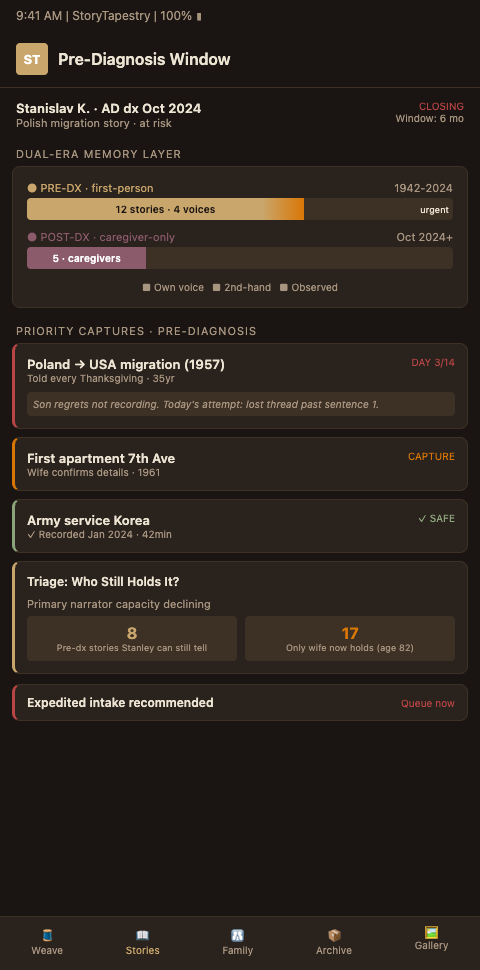
StoryTapestry's Pre-Decline Proactive Gathering feature exists specifically to close this window earlier. When a memory care facility or neurology practice refers a family to their partner funeral home at MCI diagnosis, the pre-decline story capture protocol activates before moderate-stage symptoms make direct narration impossible. The tapestry metaphor is load-bearing here: pre-diagnosis threads and caregiver-era threads weave together to produce a complete life, where either alone would produce a distorted tribute that either denies the dementia years or defines the person entirely by their decline.
SenseCams, life story books, and guided reminiscence sessions have strong evidence for preserving personal past and narrative identity (Springer - Preserving Narrative Identity for Dementia). StoryTapestry combines these approaches into a single workflow rather than requiring families to assemble multiple tools. The early-stage patient records direct narration while still able. Family members contribute corroborating stories, photos, and documents. Professional caregivers add their observations as the disease progresses. Each thread is tagged by source and era, so the final memorial can honor both the vibrant chapter before diagnosis and the different dignity of the decline years without forcing either to define the person.
Reminiscence workshops have demonstrated identity boosts even in moderate-to-severe Alzheimer's patients (Frontiers - Reminiscence Workshops Alzheimer Identity). The implication for funeral homes is that pre-diagnosis story capture does double duty: it produces material for eventual memorialization and it contributes to the patient's quality of life during their remaining cognitive years. Memory care partners who offer story capture as a therapeutic intervention while the patient can still participate are building the memorial archive without calling it that, which sidesteps the anxiety families would feel if the work were framed as funeral preparation.
The NFDA's 2024 study on digital funeral planning confirms that American families increasingly expect digital preservation options during end-of-life planning (NFDA Digital Funeral Planning Study). Pre-diagnosis story capture fits into this expectation naturally, particularly when framed as fragmented narrative building that continues throughout the disease rather than a single pre-death interview. Digital legacy planning guides recommend early story capture as a universal recommendation, not a dementia-specific one (Linkora - Digital Legacy Planning).
The referral mechanics for pre-diagnosis intake require a different vocabulary than funeral homes typically use. A family at MCI diagnosis is not ready to hear about funeral services, and the funeral home that approaches them as bereavement prospects will be refused and remembered negatively. The right framing is legacy preservation offered through the neurology practice or the memory care facility, with the funeral home's role positioned as infrastructure partner rather than service provider. Directors participating in these conversations should introduce themselves by function (legacy archivist, memorial tapestry coordinator) rather than by traditional title, and the first interaction should never include pre-need sales material. Firms that discipline themselves to this framing for the first 12 months of a pre-diagnosis program see conversion to traditional arrangement engagements 18-36 months later; firms that cannot resist pitching pre-need during the MCI window damage their referral pipeline before it develops.
Advanced Tactics for Pre-Diagnosis Story Capture
Five tactics help memory care funeral homes partner effectively with MCI and early-stage Alzheimer's care. First, structure the pre-decline intake around identity anchors rather than a complete life review. Ask about the three or four things the patient most wants remembered: the craft they mastered, the relationship they built, the community they belonged to, the values they lived. These anchors take 90 minutes to capture during a good cognitive day and provide the scaffolding that caregiver photo timelines can later populate with visual material. The anchors also guide later contributors: a family friend asked to contribute around "the community she belonged to" produces focused fragments rather than generic encomium.
Second, schedule pre-decline sessions early in the morning when cognitive performance typically peaks for Alzheimer's patients. Sundowning affects afternoon and evening lucidity even in MCI, so a 2 PM session often captures weaker material than a 9:30 AM session. Memory care facility staff can identify each patient's individual best window because they have observed it across weeks or months. Include a trusted family member in the session not as interviewer but as memory scaffold; their familiar presence keeps the patient grounded when retrieval falters and often prompts additional detail through shared reminiscence.
Third, apply the deployment chapter piecing methodology when the patient has distinct life eras that require different elicitation techniques. A veteran with Alzheimer's whose military service ended in 1974 may recall deployment details with startling clarity while losing recent-decade memories completely. The temporal gradient in autobiographical memory loss is not random; it preserves remote memories disproportionately. Pre-diagnosis capture can take advantage of this by working backward from the present, which is the direction the disease erases, so the earliest recorded material stays most accessible longest.
Fourth, build a care team handoff cadence that ensures the tapestry continues growing across clinical transitions. At MCI diagnosis the patient narrates directly. At mild-stage dementia the family members transition to primary narrators while the patient corroborates and adds fragments. At moderate-stage dementia memory care staff begin contributing sensory and routine observations while family continues adding historical context. At severe-stage dementia hospice staff contribute observation-only threads while family contributes retrospective reflection. The transitions happen gradually and should be marked in the tapestry itself, so viewers can see the care team evolving alongside the person. StoryTapestry's era-tagging makes this explicit rather than leaving it as implicit metadata only the director understands.
Fifth, respect the patient's own agency during the pre-diagnosis window. MCI patients are still capable of expressing preferences about how they want to be remembered, and the funeral home that captures these preferences directly produces memorials that feel ethically grounded. Ask the patient, while they can still answer, which stories they want included, which they want omitted, and which relationships they want acknowledged. Recorded preferences at this stage become the reference point when surrogate decisions later have to be made, and families report feeling relieved rather than burdened by having the patient's own words to guide them. A 15-minute video clip of a patient saying "I want my grandchildren to know I was more than this disease" carries weight in the later arrangement conference that no family account can substitute for, and capturing it is routine during a good morning session before moderate-stage symptoms appear.
Offer Pre-Diagnosis Capture as a Memory Care Partnership Service
Memory care funeral homes that offer pre-diagnosis story capture at MCI referral rather than waiting until bereavement position themselves as integrated partners in the dementia care continuum, not funeral vendors contacted after death. Facility administrators gain a resource for families struggling with anticipatory grief. Families receive a memorial archive that honors who the person was before the disease, not just who they became during decline. StoryTapestry provides the pre-decline intake workflows, caregiver contribution channels, and era-tagged timeline structures that make this service operationally viable. Schedule a consultation with StoryTapestry to explore how your funeral home can close the pre-diagnosis memory window for the dementia families your partners serve.
Pilot funeral homes receive direct product team support to build the referral relationships with neurology practices and memory care facilities, train directors in the legacy preservation framing that works at MCI diagnosis, and establish the care team handoff cadence that keeps tapestries growing across clinical transitions. Your first pre-diagnosis tapestries assembled on the platform receive concierge support for the full 24-month window from MCI through to eventual memorial service, which means the referral partnership is validated across the full dementia care continuum rather than at a single handoff point. Your feedback shapes the production release of the pre-diagnosis intake templates, the clinical partnership playbook, and the era-tagging structures that let families see the care team evolving alongside their loved one. Schedule a consultation to explore how your firm can close the four-to-seven-year pre-diagnosis window that most of your current memory care families are losing without realizing it.