Scaling Dementia Bereavement Programs Across Funeral Home Networks
The Scaling Paradox in Dementia Bereavement Programs
Service Corporation International operates 1,471 funeral homes across North America, controlling roughly 13% of the market in a country with 19,000 locations, 89% of which are privately owned. When SCI or a regional consolidator adds a dementia bereavement program, the question stops being "does it work at one home" and becomes "does it work at 200 simultaneously." The answer so far has been uneven.
Franchising research in healthcare delivery shows that standardization can hinder local adaptation when the service requires deep context. Memory care bereavement is exactly that kind of service: a caregiver at a rural skilled nursing facility in Ohio knows a resident's shorthand differently than a dementia-certified social worker at an urban memory-care tower in Seattle. Templatize the interview script and you lose the fragments that only local relationships surface.
The stakes are financial as well as clinical. A funeral network that invests in dementia bereavement training but achieves only 30% utilization at rolled-out branches has spent enterprise dollars for pilot-level outcomes. Consolidation is supposed to share resources — technology, vendor contracts, staff training — but the multiplier only works if the underlying program survives transplantation. Most do not survive intact.
Compounding the challenge: dementia bereavement programs depend on clinical relationships that do not exist in a spreadsheet. The branch in Cleveland that excels at memory-care partnerships has a director who spent four years building relationships with the local geriatric psychiatry clinic, the Alzheimer's Association regional chapter, and the county's three largest skilled-nursing facilities. Those relationships cannot be cloned into Indianapolis overnight. Networks that treat dementia bereavement as a product rollout rather than a relationship-weaving project discover this at branch seven or eight, usually after the launch budget is already spent.
The Tapestry Deployment Model for Network Rollout
StoryTapestry treats network scaling as a weaving problem rather than a replication problem. The enterprise defines the warp — the longitudinal threads that run through every branch: caregiver fragment collection workflow, cognitive-stage sensitive prompt library, contradictory memory reconciliation rules, pre-decline proactive gathering triggers. Individual branches then weave in the weft: their local care-facility roster, language needs, cultural practices, and staff expertise.
This split matters because phased multi-location ERP rollouts that work in 3-9 months share a common pattern: template replication for operational consistency, local configuration for contextual fit. Applied to bereavement, the warp contains the unchanging artifact — a tapestry of fragmented caregiver memories, woven into a coherent, interactive memorial. The weft contains what each branch actually collects.
Operationally, the warp is enforced through SOPs. American Franchise Academy documents how multi-unit franchises use standard operating procedures to hold quality consistent across branches. For dementia bereavement, those SOPs define the caregiver intake conversation, the cadence of pre-decline check-ins, and the rules for reconciling contradictory accounts. The actual content each branch gathers stays local.
The weft is where StoryTapestry protects local expertise. A branch that serves a Latinx population near a large memory-care network in Miami weaves in Spanish-language caregiver interviews, cross-family reconciliation protocols, and faith-community rituals. A branch in rural Vermont weaves in snowmobile-generation fragments, deer-camp stories, and neighbor-caregiver accounts. Both tapestries use the same structural grammar, but neither looks the same.
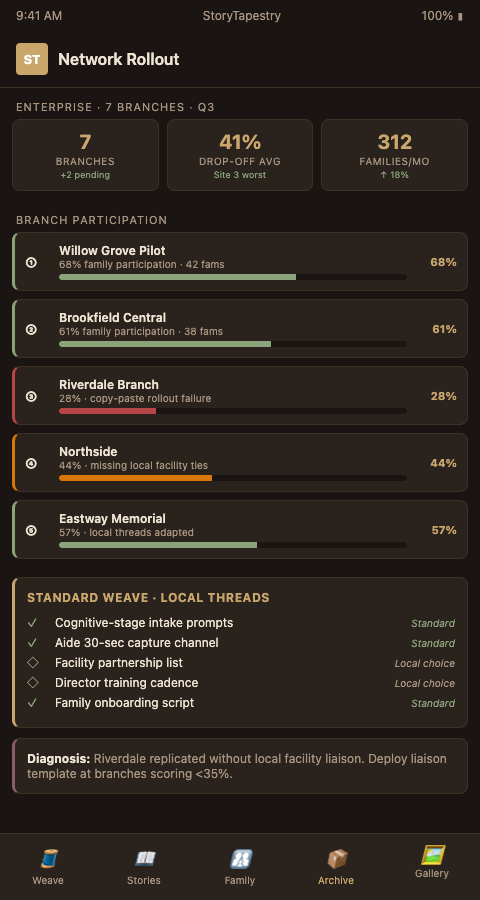
Quality control across this split follows a digital quality management approach where dashboards surface completion metrics — fragments gathered per decedent, reconciliation events resolved, pre-decline captures logged — while leaving content review at the branch level. Enterprise gets the leading indicators. Branches keep the clinical judgment.
Network rollout succeeds when the multi-site collection workflow is the thing being replicated, not the raw output. Franchise leadership often makes the mistake of benchmarking branches on tapestry length rather than tapestry fidelity. A 200-fragment memorial for a resident with late-stage dementia is usually worse than a 40-fragment memorial that survived reconciliation review. Metrics should reward the latter.
The warp specifications themselves require iteration. Enterprise teams that write the first version of the SOP from a central office discover that branches encounter edge cases the SOP did not anticipate — a spouse who is also the primary caregiver with their own early-stage MCI, a family where the legal next-of-kin lives in another country and has not seen the decedent in 12 years, a care facility that has a no-audio-recording policy that conflicts with ambient capture. StoryTapestry treats the SOP as a living document with quarterly revision cycles, drawing update proposals from branches and validating them against the four warp principles: fragment collection, stage-sensitive prompting, contradiction reconciliation, and proactive gathering. Branches that propose accepted revisions become reference sites for peer branches facing similar edge cases.
Cross-branch learning accelerates rollout. A branch that cracks a difficult partnership configuration — say, a tri-county network of small memory-care homes with no central administration — should not be an isolated success story. StoryTapestry's network dashboard surfaces these pattern wins, and enterprise rollout teams use them as templates for structurally similar branches. The logic mirrors how franchise networks share playbooks across territories: locally adapted, structurally unified.
Advanced Tactics for Enterprise Deployment
Pilot the first five branches with deliberate diversity. Do not cluster the pilot in high-performing urban markets; pick one rural, one suburban, one urban, one ethnic-majority, one multi-generational. This stress-tests the warp against the realities branches 50 through 200 will face. Pilots that only include "best case" locations hide scaling failures until they are expensive to fix.
Stagger the rollout against partner memory-care facility readiness. Every branch has an inventory of nearby assisted-living, skilled-nursing, and memory-care facilities. Score each facility on willingness to participate (does the administrator allow on-site caregiver interviews), fragment density (how many caregivers know this resident), and existing relationship (is there a discharge-planner contact). Deploy StoryTapestry first at branches whose top-three partner facilities score high across all three. Branches that score low should receive partnership outreach before technology.
Invest in regional clinical advisory boards. Three to five regional advisory boards, each pairing senior funeral directors with geriatric psychiatrists, memory-care social workers, and hospice grief counselors, create the clinical review infrastructure that a single enterprise team cannot cover. Advisory boards meet quarterly, review difficult cases flagged by branches, and propose SOP revisions that route back through the warp-update process. This structure distributes clinical judgment across the network while keeping enterprise teams focused on platform and measurement.
Build a branch-to-branch escalation channel for contradictory memory reconciliation. Late-stage dementia produces fragments that contradict one another — one caregiver recalls a decedent loved gardening, another swears she hated it, a daughter says it was the husband who gardened. Branches will handle dozens of these per month. A shared slack or Teams escalation channel where branch directors post reconciliation dilemmas creates a network-wide case library. Over 12 months, this library becomes training data for the enterprise SOP and a lived community of practice.
Tie partnership revenue models to branch performance rather than network averages. An enterprise-wide memory-care memorial package priced uniformly across branches under-monetizes high-engagement markets and over-prices low-engagement ones. Branches should set local pricing with enterprise-mandated floors and ceilings, with a revenue-share back to headquarters for platform and training costs.
Track retention of fragment-gathering staff separately from general funeral director retention. Dementia bereavement is emotionally expensive work. Branches that lose their trained fragment-gatherer lose six months of local knowledge. Protect these staff with caseload caps, quarterly reflection sessions, and salary bands that recognize the specialization. Networks that ignore this reality will see program quality decay at branches 18 months after rollout, long after the launch dashboards have stopped watching.
Build an internal certification program for branch program managers. Designate one person per branch as the dementia bereavement program lead, and require them to complete network-provided certification covering cognitive-stage prompt theory, contradiction reconciliation protocol, partnership outreach methodology, and measurement scorecard reporting. Certified leads run peer-review calls monthly, which creates horizontal knowledge sharing that corporate training departments cannot replicate. Branch leads who earn certification also become a visible career path within the network, which helps retention.
Stage enterprise technology investments around branch readiness tiers. The full StoryTapestry stack — ambient capture integration, AI threading, polyphonic memorial rendering, family portal, measurement dashboards — is more than a year-one rollout can absorb in most branches. Tier the deployment: Tier 1 at launch includes fragment collection workflow and basic interview templates; Tier 2 at month six adds AI threading and measurement; Tier 3 at month 12 adds ambient capture where facility partnerships support it. This tiering prevents feature fatigue and lets each branch consolidate competence before adding complexity.
For networks expanding across borders, the same warp-and-weft logic extends to transnational memorial scaling, where language and diaspora geography add further weft-layer variation.
Your Next Rollout Decision
Enterprise bereavement programs fail most often at branch 15, not branch 5. StoryTapestry is built for the specific scaling curve where the program must hold its clinical rigor while absorbing 200 local realities. If your network is mid-rollout and seeing participation drop at later branches, book a 30-minute rollout diagnostic with our team. We will audit your warp-weft split, surface where branches are silently deviating, and return a 90-day correction plan you can actually execute. The diagnostic includes a review of your current SOP against the four warp principles, a scorecard of three sample branches drawn from your highest and lowest utilization tiers, and a partnership-readiness snapshot for the memory-care facilities around each audited branch.
You leave the call with a one-page correction plan, a tier-mapped rollout schedule for the next six months, and a recommended certification track for the program leads you want to designate. Pilot contracts begin with five branches and a 12-week onboarding cadence, with platform access, training cohorts, and quarterly advisory-board seats included. Enterprise rollout specialists respond to diagnostic requests within two business days, and teams that choose to proceed are paired with a named implementation lead who stays through Tier 3 deployment. Bring your VP of operations, your training director, and one branch manager representing your toughest market — that trio leaves the call with aligned next steps.