Turning Sensory Fragments into Narrative Threads for Memorials
The Sensory Memory Gap in Dementia Memorials
Alzheimer's disease degrades verbal autobiographical memory faster than sensory-linked memory. Research on odor-evoked autobiographical memory in Alzheimer's patients shows that scent retrieves personal memories that verbal prompts cannot access, and the retrieval is often emotionally richer when it comes through the nose (Oxford Chemical Senses - AD Odor Memory). The limbic pathway connects scent directly to the amygdala and hippocampus, which is why the smell of a grandmother's Sunday kitchen retrieves her face when every verbal cue fails (Harvard Gazette - Scent, Emotion, Memory).
Funeral homes serving memory care families regularly encounter bereaved caregivers who know their person was still present in the final months but cannot explain how they know. The evidence is sensory: the Perry Como tears, the smile when lavender lotion was applied, the hand that relaxed at a certain voice. A study comparing visual, auditory, and olfactory cueing in Alzheimer's patients found that sensory cues consistently retrieve autobiographical memories inaccessible through direct questioning (SAGE - Sensory Cueing Autobiographical Memory AD). The challenge for memorial assembly is translating these wordless recognitions into something the service can honor.
Weaving Sensory Fragments Into Narrative Threads
StoryTapestry treats sensory fragments as primary narrative material, not supporting evidence for "real" verbal memories. The tapestry metaphor is literal here: a scent, a melody, a texture, and a taste are threads of different fibers that weave together into a memorial that captures who the person was at a multisensory level. Research on the Proust machine and the five senses confirms that autobiographical memory is encoded multisensorially and that memorials limited to verbal narration leave most of the person on the floor (Frontiers - Proust Machine Five Senses).
The intake workflow for sensory capture differs from verbal story collection. Caregivers and family members submit sensory observations in structured prompts: "What smell made her smile?" "What song triggered tears?" "What texture calmed her hands?" "What taste did she still reach for?" Each submission includes contributor attribution, approximate date, and the observer's interpretation ("I think it reminded her of her mother's bakery"). Memory care aides who spent daily time with the patient contribute the most sensitive sensory data, often observations that family members never witnessed because they came during bedtime routines or mealtimes in the facility.
Personalized music has been deployed at scale in dementia care with measurable effects. A Northwestern review of the Music & Memory program in 3,500 nursing home residents found documented improvements in agitation, social engagement, and emotional presence (Northwestern - Music as Medicine Dementia). The playlists built through programs like Music & Memory are exactly the sensory archives that StoryTapestry ingests into the memorial. When a family arrives for arrangement conferences, the facility's music preference file becomes a memorial playlist with minutes of setup rather than hours of guesswork.
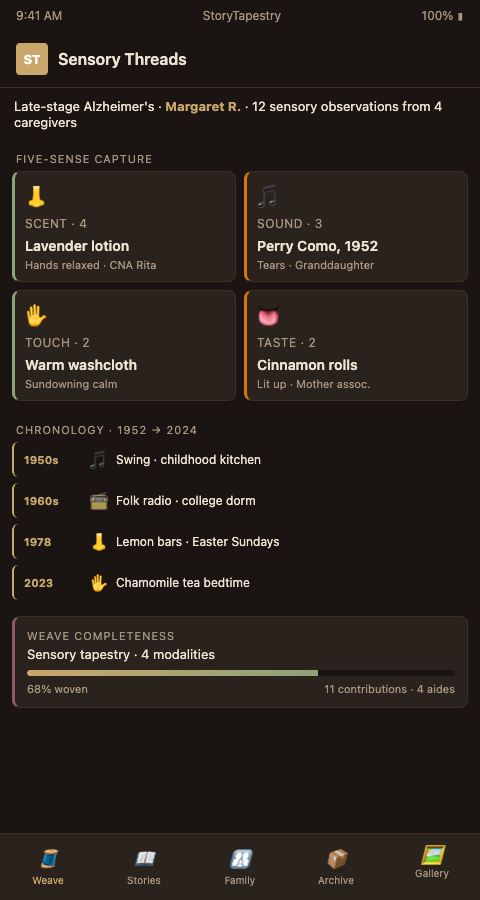
Multisensory toolkits for dementia reminiscence have been developed in research settings and translate directly to memorial contexts (Springer - Multisensory Toolkit Reminiscence). StoryTapestry's sensory intake structures four capture modalities beyond music: scent (which flowers, foods, perfumes, or environments), touch (fabrics, temperatures, textures that soothed or activated), taste (foods the patient still reached for even late in the disease), and environmental sound (birdsong, traffic, ocean, specific voices). These fragments combine with conflicting memory reconciliation to produce a memorial where sensory recognition supplements verbal narrative.
The operational reality is that facility staff witness sensory triggers constantly but rarely have a capture channel for them. An aide who notices that a patient's hands relax when given a warm washcloth is not going to stop mid-shift to document that observation in a memorial file, and by the time the patient dies the thousands of small sensory observations accumulated across caregiving years are gone. StoryTapestry's aide-facing capture channel is designed for 30-second contributions from a phone during a shift, which is the only format that actually gets used in a high-turnover care environment. The aide taps the patient's name, selects the sense modality, dictates a short observation, and is back to work in less than a minute. The cumulative archive across 12 months of these micro-contributions from four or five aides builds a sensory portrait that the family could never have assembled on their own.
Sensory material also reframes what the memorial service itself can become for dementia families. A service that plays the patient's favorite music at low volume in the lobby, sets out lavender sachets from the memory care facility's aromatherapy supply at the guest book table, and serves the cookies she baked at every church potluck is not just a funeral; it is an experience that lets mourners remember her through the same senses they remembered her by during the decline years. Directors who produce this level of sensory staging turn the service into a communal act of recognition rather than a generic farewell, and families describe these memorials as "the first time I felt she was actually in the room" in post-service conversations.
Advanced Tactics for Sensory Narrative Assembly
Three tactics transform raw sensory fragments into woven narrative threads. First, sequence sensory elements along the life timeline rather than clustering them by type. A memorial playlist that moves from 1950s swing (childhood home) to 1960s folk (college years) to 1970s soft rock (early marriage) to hymns (her final facility years) tells a life story in sound. A memorial that just plays every song she liked in alphabetical order tells nothing. StoryTapestry's sensory timeline enforces chronology automatically when families provide era anchors.
Second, pair sensory fragments with visual memory prompts during story elicitation sessions. A caregiver who cannot remember verbal stories often produces rich narrative when handed a photo alongside the patient's signature scent (a vial of lavender oil from the memory care facility's aromatherapy supply). The cross-modal cue retrieves material that either cue alone would miss. This is a well-documented technique in reminiscence therapy that transfers directly to memorial assembly.
Third, extend sensory capture to perinatal and obstetric bereavement contexts when the memory care patient was also a grandparent who never met a deceased grandchild. Ultrasound heartbeat tapestry techniques from perinatal memorial programs inform how StoryTapestry handles sound fragments in general: a fetal heartbeat recording and a patient's last hummed melody are both sonic memory artifacts that require similar preservation logic. Funeral homes with both memory care and perinatal partnerships benefit from unified sensory infrastructure.
Fourth, distinguish between comfort sensory triggers and activation sensory triggers in the capture taxonomy. A scent that calmed a patient during sundowning agitation belongs in a different memorial context than a scent that activated happy excitement during good cognitive windows. Both are real, both matter, but using them interchangeably produces a confused memorial experience. The family's grandmother who relaxed into sleep with chamomile tea and lit up at the smell of her mother's cinnamon rolls should have both scents represented but positioned differently in the service: the chamomile near the reflective guest book area, the cinnamon near the opening reception where mourners gather energetically. StoryTapestry's sensory tags include a valence field (comfort, activation, neutral) that guides directors toward sensory staging decisions that honor the actual emotional textures rather than blending them into a generic sensory atmosphere.
Fifth, treat the deceased's own sensory preferences as primary and the family's sensory associations as secondary. A daughter who associates her mother with lemon bars because she always baked them for Easter dinners may want lemon at the service, but if the mother herself preferred the smell of fresh bread and found lemon too sharp in her final years, the director should gently surface this tension. The memorial exists to honor the deceased, not to comfort the bereaved with projections; when there is a choice, the deceased's preferences win. StoryTapestry's intake distinguishes patient-sourced and family-sourced sensory associations so the tension is visible rather than invisible, and directors who facilitate this conversation report that families ultimately prefer the deceased-centered choice even when they initially advocated for their own association.
Equip Your Memory Care Services With Sensory Memorial Capabilities
When your funeral home can translate sensory fragments into woven narrative threads, the memorials you produce for memory care families honor what families actually experienced during the disease years, not just what can be reduced to paragraphs. Families whose caregivers witnessed late-stage Perry Como tears and lavender lotion recognitions feel seen by a funeral service that includes these elements, and they refer other families from the same facility networks. StoryTapestry provides the sensory intake workflows, timeline sequencing, and cross-modal capture tools that turn these capabilities into operational strengths. Contact StoryTapestry to discuss how memory care funeral homes can add sensory narrative threads to their memorial offerings.
Pilot memory care funeral homes receive product team support to onboard facility aides to the 30-second sensory capture channel, train directors on five-sense intake sequencing during arrangement conferences, and coordinate with facility life enrichment programs already running music and aromatherapy interventions so the memorial archive ingests their observation records rather than duplicating their work. Your first sensory memorials on the platform receive concierge support including on-site sensory staging consultation for the service itself, with the product team helping the director select which scents belong in which room and which audio elements support which moments of the service. Your feedback shapes the production release of the aide-facing capture channel, the valence tagging structure, and the sensory staging templates that transfer the archive from collection to service experience.
Schedule a consultation to discuss how your firm can move sensory narrative from a rare flourish in a handful of memorials to a standard capability across every memory care family your facility partners refer to you.