Funding Models for Hospital-Based Infant Memorial Programs
The Sustainability Problem in Hospital Infant Memorial Funding
A maternal-child health director at a 300-bed community hospital secured a three-year grant from a regional foundation to launch a perinatal bereavement program with a dedicated coordinator, memory-making supplies, and staff training. The program flourished. Family feedback improved. Clinician retention in L&D increased. Year four arrived. The grant had been time-limited. The hospital operating budget did not absorb the program. The coordinator transitioned to another role. Memory-making supplies ran down. Training lapsed. By year five, the program existed only in the filing cabinet with the grant application.
The research documenting time-limited grants facing sustainability challenges establishes that grant-funded launch without institutional absorption is the most common failure pattern in perinatal bereavement infrastructure. The cost-utility evaluation of online bereavement programs demonstrates that bereavement programs can be economically evaluated with rigor, yet most hospital programs lack the economic framing that secures operating budget commitment. Funding sustainability is not primarily a generosity problem. It is an architecture problem.
Hospital infant memorial programs face a specific funding challenge: they are clinically essential but rarely revenue-generating in traditional fee-for-service terms. They reduce complicated grief, improve clinician retention, and strengthen community reputation. These outcomes are real but do not appear in standard hospital revenue cycles. Without deliberate funding architecture, the program depends on the passion of its current champion.
The StoryTapestry Framework for Sustainable Memorial Program Funding
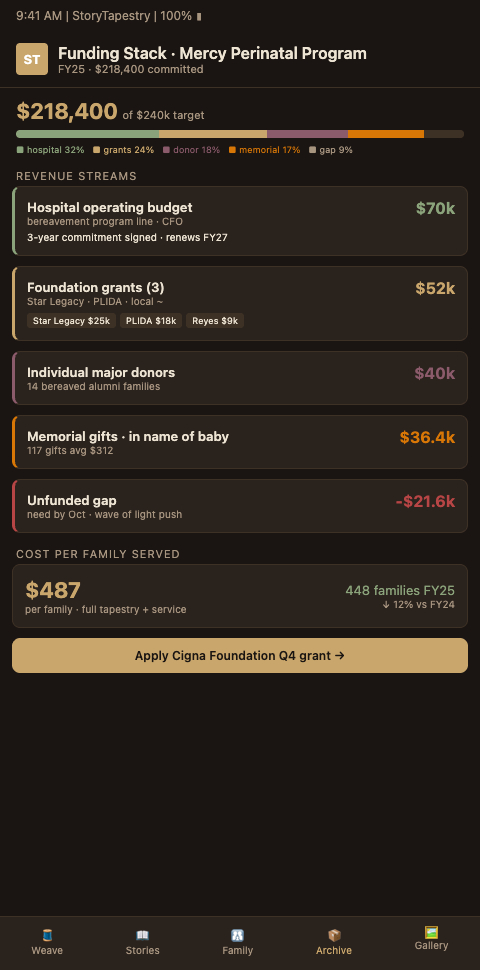
StoryTapestry treats program funding the way a master weaver treats a multi-year commission: the income stream across a long project requires diverse sources, structured milestones, and transparent accounting of how each thread of funding maps to each phase of the work. The framework builds a funding tapestry across four income categories rather than depending on any single thread.
Funding category one is hospital operating budget commitment. This is the load-bearing warp thread. Operating budget absorption requires framing the program as clinical infrastructure with documented outcomes, not as a discretionary wellness offering. Programs that measure outcomes using validated grief instruments and engagement analytics from hospital program scaling rollouts build the evidence base that persuades finance committees. Programs that present satisfaction surveys alone do not.
Funding category two is competitive grant funding. The NACG Grief Reach Grants annual cycle supports grief programs nationally. The Beckwith Institute perinatal loss funding program specifically funds perinatal loss projects. The Foundation for Grieving Children grants to 501(c)(3) organizations supports children's grief programming that intersects with sibling inclusion. These grants typically run 12 to 36 months and work best when framed as expansion or innovation funding on top of a stable operating budget foundation rather than as the foundation itself.
Funding category three is hospital foundation philanthropy. Most hospital foundations accept designated gifts for specific programs. A perinatal bereavement program with clear naming opportunities, such as a named coordinator position, a named memory-making program, or a named annual remembrance event, attracts grateful families and community donors. The TEARS Foundation funeral assistance program covering babies 20 weeks through age 1 demonstrates the donor appetite for perinatal loss philanthropy when clear giving pathways exist.
Funding category four is partnership revenue. StoryTapestry offers hospitals a licensing model that can be reimbursed in part by family memorial package purchases, funeral home partnership revenue, and payer-aligned wellness reimbursement where available. This partnership thread typically covers 15-30% of program cost at maturity, complementing rather than replacing other funding categories.
The tapestry metaphor matters because no single funding thread supports the full program. Hospital operating budget provides stability. Grants provide innovation capacity. Philanthropy provides community connection. Partnership revenue provides operational reduction. When all four threads weave together, the program survives budget pressures that would sever any single thread. The ProPublica nonprofit tax filings structure for bereavement organizations demonstrates how mature bereavement nonprofits structure their finances, offering templates for hospital-affiliated programs.
Programs that achieve funding sustainability benefit from integration with hospital program scaling approaches that unlock network-level grant scale, OB unit funeral referrals that generate partnership revenue, and memorial partnership revenue frameworks that have been proven in memory care contexts and transfer to perinatal settings.
The four-category tapestry has a practical sequencing implication. Programs that launch with grant funding first — the most common pattern — face the sustainability problem at year three when the grant ends. Programs that launch with operating budget commitment first, even at a reduced scope, and layer in grants as expansion funding tend to survive the grant cycles without trauma. The sequencing matters because operating budget lines, once established, are harder to remove than to create; a program that has been in the operating budget for three years has a political foothold that a grant-funded program does not. Bereavement coordinators negotiating program funding with their CFO should accept a smaller operating budget line in year one in exchange for the stability that line provides, and use grants and philanthropy to expand the program from that stable base rather than to launch it.
The second sequencing implication concerns philanthropy. Hospital foundations cultivate donors over years, not months. A program that announces a named coordinator position in year one, with no donor relationships in place to support the naming, is unlikely to find the donor before the year-one budget cycle closes. Programs that begin philanthropic cultivation eighteen months before they expect to need the funding — quietly, through conversations with foundation staff about community need rather than through solicitation for a specific program — tend to surface donors when the program is ready to receive them. This is foundation infrastructure work that the bereavement coordinator cannot do alone; it requires active partnership with the hospital foundation's director of development and typically a one-hour monthly check-in across a two-year cultivation window.
Partnership revenue is the category most programs under-invest in. Hospital bereavement programs often assume partnership revenue means "fees from families," which feels extractive in a bereavement context. The actual revenue streams are broader: licensing fees from affiliated funeral homes who use the hospital's tapestry integration as a service differentiator, reimbursement from payers who have wellness-benefit lines for bereavement care, and co-marketing revenue from memorial photography vendors who gain access to the hospital's family cohort through the partnership. Each of these streams requires negotiation infrastructure — legal review, contract templates, revenue share agreements — that single-site programs rarely have the capacity to build. Networks that build this infrastructure once and share it across sites unlock partnership revenue that single sites cannot reach.
Advanced Tactics for Securing and Sustaining Memorial Program Funding
Programs that achieve long-term sustainability follow four tactical patterns that grant-to-grant programs typically neglect.
Build outcome measurement before applying for any grant. Grantmakers increasingly require pre-specified outcome measures, logic models, and evaluation plans. Programs with PGIS baseline, 6-month, and 12-month administration protocols, clinician retention tracking, and family experience scores in place before grant application secure funding faster and at higher amounts than programs that promise to develop measurement during the grant period. Measurement infrastructure is not a grant deliverable. It is a grant prerequisite.
Cultivate donor relationships intentionally, often routed through the same OB unit funeral referrals pathways that already connect families to downstream services. Hospital foundations receive gifts from families whose children survived. Perinatal memorial programs must build equivalent pathways for families whose children did not. This requires careful navigation: bereaved parents should never feel solicited during acute grief. Programs that send structured invitations 18-24 months post-loss for grateful families to share their stories, and separately introduce philanthropy opportunities only when families express readiness, build durable donor relationships without transactional feel.
Pursue multi-year funder relationships rather than one-off grants. Regional foundations often prefer funding one program across three or four grant cycles rather than funding a new program each cycle. Programs that report back on outcomes, document lessons learned, and invite funders into program development become repeat grantees. Single-transaction grantseeking produces unstable funding.
Plan for institutional transitions, borrowing continuity patterns from memorial partnership revenue work in memory care networks where leadership turnover is equally common. Hospital CEOs change. Chief nursing officers rotate. Foundation executive directors retire. Programs that survive leadership transitions have documented value propositions, outcome evidence, and community advocacy that does not depend on any single institutional champion. Transition planning is a quarterly discipline, not an annual report.
Structure the budget narrative for finance committee audiences. Bereavement coordinators presenting to CFOs or finance committees often lead with mission language — the families served, the grief reduced, the community built. Finance committees need this context but cannot act on it alone. The budget narrative should frame the program as clinical infrastructure with three quantified outcomes: reduced clinician turnover in L&D and NICU units (with retention-cost data), reduced emergency department utilization by bereaved families at 3, 6, and 12 months (with per-encounter cost data), and improved hospital reputation scores that correlate with maternity service line volume. Programs that translate their mission into these three outcome categories secure operating budget commitments that mission-only narratives do not.
Separate program costs from platform costs in funding applications. A common error in grant applications is bundling platform licensing, training, memory-making supplies, coordinator salary, and chaplaincy time into one line item. Grantmakers often fund program expansion but decline to fund platform licensing, assuming the institution should carry technology costs. Applications that break costs into clearly labeled categories — platform infrastructure (institutional responsibility), program expansion (grant-eligible), family-facing supplies (grant-eligible), staff training (partially grant-eligible), research evaluation (grant-eligible) — align with grantmaker funding logic and secure approvals that bundled budgets do not.
Build a donor communication cadence that honors the families behind the philanthropy. Hospital foundations often want gratitude from bereaved families directed to donors. Bereavement coordinators must hold the line: bereaved families are never asked to write thank-you notes, attend donor events, or share their stories on a foundation's timeline. Families who want to share may do so at their own initiative, typically eighteen to thirty-six months post-loss, and the foundation's donor communication strategy must accommodate these long timelines. Programs that rush the family-to-donor communication cycle damage trust with both families and foundation partners. Programs that wait produce donor relationships that last decades because donors understand they are funding care at the pace of grief rather than the pace of marketing.
Build Funding Architecture That Sustains Your Memorial Program
Hospital bereavement programs that want to move from grant-cycle anxiety to durable funding architecture can partner with StoryTapestry's program development team. We work with hospital administrators, foundation staff, and clinical leadership to map the four-category funding tapestry, build outcome measurement infrastructure, secure competitive grants, cultivate philanthropy pathways, and structure partnership revenue.
Request a funding architecture consultation to map your current funding mix against sustainability benchmarks and identify the threads your program is missing to survive the next budget cycle with strength rather than worry. The consultation includes a five-year funding projection that models your program across the four categories, a gap analysis that identifies which threads are over-concentrated or missing, and a phased funding strategy that diversifies the program's income without disrupting current operations.
Bring your bereavement coordinator, a representative from your hospital foundation, and — if possible — a member of your finance team to the consultation. The combination of programmatic, philanthropic, and financial perspectives in the same conversation produces funding architecture that is actually buildable within your institution's existing governance rather than a theoretical framework that stalls when it meets the CFO's approval process. Programs that survive budget cycles for a decade or more did not get there by accident; they built multi-category funding architecture deliberately, often with external advisory support, and they maintained that architecture as a discipline rather than a one-time project.