How OB Units Can Streamline Funeral Memorial Referrals
The Referral Gap at the Obstetric-Funeral Interface
A bereavement coordinator at a Level III maternity unit reviewed exit paperwork given to families after perinatal loss. The packet contained a photocopied list of 23 funeral homes in the surrounding three counties, a generic grief resource brochure from 2009, and a single page with the hospital chaplain's name and a phone number that had rung through to voicemail during her test call. The packet had not been updated in four years. No warm handoff existed. Families left the hospital with paper and a recommendation to "call when you're ready."
The ACOG management of stillbirth guidance recommending bereavement counselor referral establishes clear standards for referral practice. The bereavement care guidelines research documenting organizational responsibility for post-discharge referrals confirms that referral coordination falls to the healthcare organization, not to the bereaved family. Yet implementation inconsistency is pervasive. A family making decisions about funeral arrangements in the 48-72 hour window after loss cannot evaluate 23 funeral homes cold. They need a coordinated handoff.
The gap between ACOG guideline and discharge reality represents a translation failure from clinical consensus into operational workflow. Funeral homes, bereavement counselors, pastoral care staff, and OB units typically operate as separate entities with no structured referral protocol. Families bear the coordination burden during the worst week of their lives.
The operational consequences compound. A family calls five funeral homes from the photocopied list before finding one that handles infant losses at any gestational age. Two homes quote burial fees without mentioning the waived infant-burial rates they actually offer. Another declines because the family mentions an early-gestation loss. By the time the family identifies a funeral home ready to serve them, 72 hours have passed and the hospital has already transferred the baby to the county medical examiner's holding facility. The discharge packet created this entire sequence by outsourcing the coordination work to a family in acute grief. OB units that accept the coordination responsibility convert this failure pattern into a 24-hour warm handoff. The difference shows up in family experience scores, in timely burial placement, and in the partnerships funeral homes build back toward the hospital for future pre-need conversations.
The StoryTapestry Framework for OB Unit Funeral and Memorial Referral Streamlining
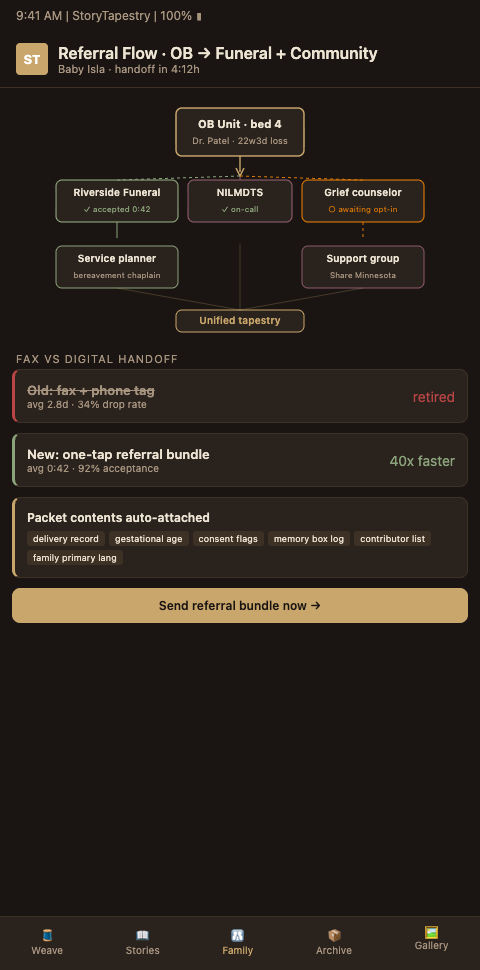
StoryTapestry approaches referral workflow the way a master weaver approaches the point where one tapestry ends and another begins: the transition must be seamless, with threads carrying through without unraveling, and the weaver who takes over must know exactly which pattern is in progress. The framework formalizes three handoff layers that replace the photocopied funeral home list with coordinated transition.
Handoff layer one is the internal hospital team transition, which builds on the hospital funeral handoffs protocol foundation. Before the family leaves L&D, a structured transition occurs between the L&D nurse who cared during delivery and the bereavement coordinator or social worker who will manage post-discharge coordination. The transition includes tapestry access, family preference documentation, and outstanding memory-making tasks. The Mount Sinai multidisciplinary perinatal bereavement program demonstrates how social workers, chaplains, and OB staff can operate as a coordinated team when infrastructure supports it. The AWHONN bereavement coordinator template role description offers a formal definition of the coordinator role that makes handoff expectations explicit.
Handoff layer two is the funeral home and memorial service referral. Rather than handing families a list of 23 funeral homes, the platform presents a curated network of funeral partners that have completed perinatal bereavement care training, understand infant funeral logistics (including small casket arrangements, infant-appropriate ceremonies, and financial assistance options), and commit to specific response times. Families select from three to five vetted partners with profile information about each. The selected funeral home receives a structured referral with the family's contact preferences and tapestry access, subject to family consent. The cost-neutral chaplain and social worker bereavement pilot research demonstrates that coordinated referral pilots can operate without new staffing.
Handoff layer three is the ongoing bereavement support referral. The platform integrates referrals to grief counseling, support groups, and peer connection opportunities matched to the family's preferences. The perinatal palliative care pathway integration research confirms that pathway integration enables specialist support that isolated referrals cannot. The seamless care research on integrative perinatal palliative care models supports integrated referral as a core operational pattern.
The tapestry metaphor holds throughout because the same memorial tapestry travels with the family. The L&D nurse who contributed threads during delivery, the bereavement coordinator who contributes during the post-discharge window, the funeral home that may contribute ceremony threads, and the grief counselor who supports ongoing engagement all weave into the same tapestry rather than producing parallel disconnected records. The family's experience is of continuous care rather than fragmented handoffs.
Referral streamlining integrates with adjacent infrastructure: hospital funeral handoffs establishes the protocol foundation, L&D staff training ensures that nurses know how to initiate the handoff properly, and partnership referral programs across cultural associations demonstrate how referral networks can extend beyond funeral homes into community partners that serve specific populations.
The three handoff layers need different response times and different personnel. Layer one — internal hospital team transition — happens within the hospital stay and must be coordinated in real time, often with the bereavement coordinator on-call overnight to receive the handoff. Layer two — funeral home referral — happens in the 48-72 hour window after loss and must accommodate the family's emotional capacity in that window, which means offering three to five vetted options rather than 23 cold listings. Layer three — ongoing bereavement support — unfolds across months and years, with referral prompts timed to specific grief milestones rather than offered in a single packet at discharge. Programs that treat all three layers as one event at discharge collapse the protocol back into the original problem: paper handed to a family during the worst week of their lives.
The curated partner network needs a geographic structure the family can actually navigate. A mother who lives thirty miles from the hospital and forty miles from her baby's father's family should not be forced to choose between a funeral home near the hospital and a funeral home near her extended family. StoryTapestry's partner network is organized by both hospital catchment and family residence, so a family can receive options that serve multiple geographic anchors in their life. The coordinator filtering the options sees the family's addresses, the funeral homes that serve those addresses, and the subset that has completed perinatal bereavement certification. The filter typically narrows 23 regional funeral homes to four or five that actually serve the family's specific situation, which is the level of curation families can process during acute grief.
Bilingual coordination is the hidden variable in referral quality. A hospital serving a significant Spanish-speaking population that partners only with English-primary funeral homes produces handoffs that technically complete but leave families carrying translation labor during the funeral planning. Partner network curation must include language capacity as a first-class filter. Families are offered funeral partners who can hold the planning conversation in the family's preferred language, and the referral packet is translated to match. This is not a nice-to-have; for many families it is the difference between an arranged funeral and a funeral the family did themselves without institutional support because the referral felt too foreign to accept.
Advanced Tactics for Sustained Referral Network Quality
Programs that build referral networks and then watch the network decay into outdated partner lists miss the network maintenance tactics that distinguish high-quality coordination from nominal coordination. Four tactics sustain referral quality across time.
Audit partner network quarterly. Funeral home ownership changes. Counselor practices relocate. Pastoral care contacts retire. A referral network that is not audited quarterly becomes unreliable within 18 months. The audit should confirm current contact information, verify that perinatal bereavement care training is current, review the past quarter's family feedback, and identify gaps in geographic or cultural coverage.
Build partner onboarding requirements that protect family experience, modeled on the same rigor applied to L&D staff training curricula. New funeral home partners must complete perinatal bereavement care training, provide current liability insurance documentation, commit to infant funeral logistics capability including small casket arrangements and infant burial plot coordination, and accept the platform's documented response time standards. Partners who fulfill requirements receive network access. Partners who do not, do not, regardless of geographic convenience.
Collect structured family feedback about referral experiences. Two weeks after funeral arrangements complete, families receive a brief structured feedback form about the referral process, the funeral home experience, and ongoing coordination quality. Feedback is reviewed monthly and informs network decisions. Partners whose feedback trends negative receive support or network removal. Feedback that is uniformly positive despite obvious gaps indicates survey design problems rather than perfect care. The research on connecting families to bereavement resources supports structured feedback as the backbone of quality referral practice.
Extend the network across geographic reality by integrating partnership referral programs from cultural associations that serve specific diaspora communities. Families rarely live exclusively in the hospital's immediate catchment area. The referral network must cover the regions where families live, work, and have extended family, not only the three blocks surrounding the hospital. Multi-site networks, often coordinated across hospital system scale, make this geographic extension practical rather than aspirational.
Build referral feedback into the coordinator's quarterly review cadence. A bereavement coordinator who reviews referral outcomes quarterly — which partners families chose, which completed services without incident, which produced family complaints — notices patterns that never surface in annual audits. A funeral home that receives 40% of a quarter's referrals and produces one complaint may be acceptable; a funeral home that receives 10% of referrals and produces three complaints is not. Quarterly review pace catches the small patterns before they become reputational issues. The review should be structured: partner name, referral count, completion rate, family-reported experience score, coordinator-reported friction, and recommended network status. This structure makes the review transferable across coordinator transitions.
Coordinate ongoing bereavement support referrals with the family's consent preferences. Some families want active outreach at 2, 6, and 12 weeks; some want coordinator contact available but no proactive outreach; some want no institutional contact after services conclude. StoryTapestry captures these preferences at intake and routes referrals accordingly. Default should be the family's stated preference, with gentle annual check-ins for families who requested them.
Handle families whose chosen funeral home falls outside the network. A family may have a relationship with a funeral home the hospital has never partnered with — a director who served a grandparent, a congregation tied to the funeral home's owner, a family business across generations. StoryTapestry's self-service onboarding flow for out-of-network funeral homes completes in about 30 minutes, includes core perinatal bereavement training modules, and grants time-limited tapestry access. The platform extends the coordinator's reach to include the family's choice rather than forcing the family to fit the network.
Document the referral pattern for executive reporting. Leadership often asks coordinators to quantify referral activity. A coordinator who produces monthly reports — families referred, partners used, completion rates, family experience scores, geographic reach — demonstrates program value in the operational language finance and quality committees recognize.
Streamline Your OB Unit's Funeral and Memorial Referral Workflow
Hospital OB units that want to move from photocopied funeral home lists to coordinated referral infrastructure can adopt StoryTapestry's referral network module. The module handles internal team handoffs, funeral partner vetting and coordination, and ongoing bereavement support referrals with integrated tapestry continuity across every handoff. Our referral network team works with hospital OB leadership, social work departments, and regional funeral partners to build and maintain the network over time.
If your unit's current referral process rests on paper lists and hope, request a referral workflow consultation to design the coordinated pathway that meets ACOG guidance and serves families during the worst week of their lives. The consultation includes a review of your current referral packet, an audit of your existing partner network for currency and capacity, and a recommended rollout plan for the three-layer handoff model tailored to your unit's patient population and staffing.
Bring your OB medical director, your bereavement coordinator, and a representative from your social work team to the consultation. If possible, invite one or two partner funeral directors who serve your unit most often. The combination of medical, bereavement, social work, and funeral perspectives in the same room produces a referral protocol that actually works across the transitions families make, rather than a protocol designed for only one handoff point. Most units can move from the photocopied-list baseline to a coordinated three-layer protocol in six to nine months, with the first three months focused on internal handoff and partner vetting, and the following months extending into ongoing bereavement support integration.