5 Ways Hospital Bereavement Teams Can Support Digital Memorials
The Problem: Bereavement Teams Ship Memory Boxes, Then Lose Contact With Families
A perinatal bereavement coordinator in a 400-bed community hospital told us she tracks about 180 families per year. Her team assembles memory boxes, arranges mold castings, and coordinates chaplaincy when requested. But seventy-two hours after discharge, 80% of those families disappear from her tracking. The bereavement follow-up call at six weeks reaches about half. The annual memorial service draws a few dozen of the 180. The rest — the vast majority — return to a world that has moved on, carrying fragmented memories with no platform to hold them.
This pattern is documented. A scoping review of bereavement care guidelines identified the appointment of a dedicated bereavement coordinator as one of the highest-impact improvements a perinatal unit can make — but noted that even coordinator-led programs struggle with post-discharge continuity. AWHONN's perinatal bereavement certificate program trains interprofessional teams in interventions that work during admission; the gap opens after the family goes home. Mount Sinai's bereavement program model explicitly extends to parents, siblings, and grandparents — demonstrating that best-practice hospital teams already understand the need, even when they lack infrastructure.
The bereavement team's problem is not clinical. It is logistical: there is no connective tissue between the memory box handed over at discharge and the ongoing grief that unfolds across months and years.
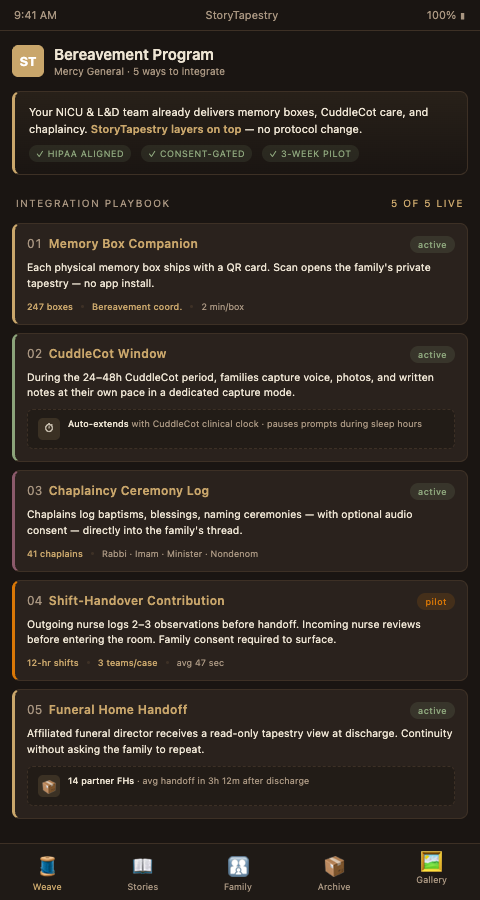
The Solution: Five Integration Points Where StoryTapestry Weaves Into Existing Bereavement Workflows
StoryTapestry does not replace bereavement teams or their protocols. It functions as a digital loom onto which existing care practices feed their threads. Hospital bereavement coordinators using StoryTapestry describe it as the first tool that makes the months after discharge as structured as the hours during admission. Here are five specific integration points where the tapestry extends work teams already do.
1. Memory Box Digital Companion. When a bereavement nurse assembles a memory box, every physical artifact — the footprint card, the lock of hair, the blessing beads — can be photographed and entered into a matching digital tapestry. Families leave the hospital with both the physical box and a private link to a tapestry already seeded with those exact artifacts. The humanized care protocol literature documents that CuddleCot usage, memory boxes, and immediate support are all more effective when accompanied by post-discharge continuity — StoryTapestry provides that continuity as a digital thread from the first hour.
2. Chaplaincy and Blessing Ceremony Documentation. Hospital chaplains lead baptisms, blessings, and naming ceremonies that the extended family cannot attend. StoryTapestry integrates with chaplaincy workflows so that the exact words of a blessing, the name the chaplain spoke, and (with consent) an audio recording of the ceremony all become tapestry threads. A grandmother in Manila watching a grandchild's blessing from a phone becomes part of the ceremony via the shared tapestry view.
3. NICU Nurse Observation Handoff. NICU palliative and bereavement care models describe a family-centered integrative approach where multiple shifts of nurses each carry pieces of the family's experience, and disciplined NICU nurse story capture is how those pieces stop disappearing between shifts. StoryTapestry provides a shift-handover channel where nurses can add observations before logging off, always subject to family consent before public display. A 36-hour NICU stay that involves eight nurses now produces eight contribution threads rather than one generalized discharge summary.
4. Post-Discharge Anniversary Touchpoints. Bereavement coordinators already know the calendar dates families will need support: the six-week check-in, the three-month anniversary, the first Mother's Day, the due date, the birthday. StoryTapestry automates gentle, skippable prompts on each of these dates — not asking for more content, but inviting families to re-visit the tapestry, add a new reflection if they wish, or simply sit with what is already there. Share's support infrastructure already models this long-tail engagement; StoryTapestry extends it to the hospital-affiliated context.
5. Affiliated Funeral Home Continuity. Hospitals increasingly partner with specific funeral homes that specialize in perinatal services. StoryTapestry links the hospital bereavement tapestry directly to the funeral director's workflow, preserving continuity from ICU to service to ongoing memorial. The funeral director's contributions — the order of service, the selected readings, the eulogy text — all become tapestry threads the family can revisit forever. This mirrors the facility bereavement partnerships approach we support across other care settings.
These five integration points share a common design principle: each one attaches to an existing bereavement workflow rather than adding a new one. A coordinator managing 180 families per year cannot absorb a separate digital system on top of her memory box assembly, chaplaincy scheduling, and discharge paperwork. The tapestry layer sits inside the work she already does. When she photographs a mold casting for the memory box, the photograph lands in the tapestry automatically. When she schedules a chaplain for a 2am blessing, the chaplain's scheduling note becomes the backbone of a tapestry thread that the family completes at their own pace. The administrative load does not double. It shifts from disposable documentation to archival documentation, and the archival version is what the family carries home.
The second design principle is revocability. Every tapestry thread the hospital creates can be removed, edited, or hidden by the family at any time. A nurse's shift-handover observation that feels comforting at 72 hours may feel intrusive at twelve weeks; the family can retire the thread to a private vault with one action, and the nurse's contribution survives in the archive even when it no longer appears in the public weave. This matters because bereavement coordinators are often asked, "what if my family regrets what the hospital captured?" The answer is that the family owns every thread, can retire any thread, and can restore any retired thread. The hospital's role is to offer threads, never to impose them.
Advanced Tactics for Bereavement Team Integration
Pre-admission tapestry opening for known lethal diagnoses. When a family receives a fatal prenatal diagnosis at 20 or 22 weeks, bereavement coordinators can open a tapestry during pregnancy. Parents add ultrasound videos, name candidates, letters to the baby, and recorded conversations — all before delivery. This preparation reduces the cognitive load at the moment of loss and produces a tapestry that begins with pregnancy rather than admission. Resolve Through Sharing's curriculum for 65,000+ trained professionals already models pre-admission preparation as best practice.
Interdisciplinary team rounds documentation. The weekly interdisciplinary rounds in NICU and OB units produce observations that rarely reach families directly, and the same principle underpins our doula and birth worker contributions outside the hospital walls. StoryTapestry includes a team-rounds capture mode where clinically relevant, family-appropriate observations can be drafted, reviewed by the bereavement coordinator, and offered to the family as potential tapestry threads they can accept or decline.
Research participation bridging. Many perinatal bereavement programs run research studies on grief trajectories and care outcomes. StoryTapestry can, with explicit consent, provide de-identified structural data (number of contributions, timing patterns, family engagement duration) to IRB-approved research without exposing any narrative content. Coordinators gain longitudinal data about their program's impact without burdening families with separate research instruments.
Translation and language inclusion. Hospital bereavement programs increasingly serve multilingual communities. StoryTapestry's prompts and display support translation that preserves the exact words of each contributor — a Vietnamese grandmother's blessing stays in Vietnamese, with a translation appearing on request. No family loses its voice to the bereavement program's dominant language.
Staff wellbeing reflection space. The secondary trauma that NICU and OB staff carry is well-documented, and the structural parallels with care facility bereavement partnerships in the memory care space are informative for hospital programs. StoryTapestry provides a separate, clinician-only reflection space tied to each case — entirely private from the family — where nurses, residents, and chaplains can process what they witnessed. Bereavement coordinators can aggregate anonymized staff reflections for team support without breaching family confidentiality.
Morbidity and mortality conference integration. Perinatal units run M&M conferences where clinically complex cases are reviewed for learning. These conferences typically reduce a family to a slide of timestamps and clinical milestones. When the family has consented, StoryTapestry provides a family-facing summary that can be shared with the M&M committee so that the review honors the child as a person rather than a case number. This is not a substitute for clinical review; it is a reframe that keeps the humanity of the loss present during the technical analysis. Nurse managers report that M&M conferences following this model produce more constructive quality improvement conversations because the staff in the room remember why the work matters.
Cross-shift consent continuity. A family's consent preferences captured on admission at 11pm on a Friday must survive handoff to the weekend team, the Monday daytime staff, and the next month's bereavement coordinator. StoryTapestry stores consent as structured data attached to each tapestry thread, visible to every clinician with access, with timestamp and version history. A family who said "no photographs of his face" at admission has that preference respected at every subsequent interaction, and a family who changes their mind at 36 hours has the new preference propagate immediately. This removes the "I forgot what they wanted" failure mode that produces the most painful bereavement complaints.
For Hospital Bereavement Teams Ready to Extend Their Reach
Your bereavement program already does remarkable work. StoryTapestry is the infrastructure that carries that work into the months and years your team cannot staff. We integrate with your existing consent practices, EHR documentation, chaplaincy workflows, and affiliated funeral partnerships. Coordinators who pilot StoryTapestry typically begin with one unit — usually NICU or labor and delivery — and expand once their team sees the reduction in lost continuity. The same tapestry infrastructure supports NICU medical staff stories capture, doula birth worker roles documentation, and broader bereavement partnerships.
A typical pilot runs 90 days with a cohort of ten to fifteen families, shadowed by the bereavement coordinator and reviewed in a final session with the nursing leadership, a hospital compliance officer, and the two or three funeral home directors most frequently chosen by families in the unit's catchment area. The pilot produces three artifacts: a workflow map showing how tapestry contributions fit inside existing shift structures, a consent template reviewed by your compliance office, and a set of de-identified family feedback scores comparing the cohort's six-week and twelve-week engagement to the unit's historical baseline.
Reach out to schedule a discovery conversation with your nursing leadership and affiliated funeral home partners. We will review your current memory box protocol, your chaplaincy scheduling workflow, and your post-discharge follow-up calendar, and map the five integration points onto your existing infrastructure. Most programs find that two or three of the five integration points are immediately feasible, with the remaining two requiring modest workflow adjustments that can roll out in the second quarter of adoption.