Coordinating Between Obstetric Units and Bereavement Counselors for Story Capture
The Problem: Bereavement Coordination Held Together by Individual Heroics
Perinatal loss happens across several hospital units — labor and delivery, NICU, antepartum, postpartum, maternal-fetal medicine, postmortem — and the people who know the family best at any given moment shift rapidly. A review in ScienceDirect on meeting challenges in perinatal bereavement concludes that cross-unit collaboration between L&D, NICU, and pastoral care improves family outcomes, but also documents that most hospitals lack formal coordination protocols. Individual nurses decide, case by case, whether to page bereavement, whether to call a chaplain, whether to start memory-box preparation, and the decisions reflect their own training and tenure rather than a unit standard.
A Springer chapter on interdisciplinary team approach to pregnancy loss describes the ideal team composition — OB, nursing, social work, pastoral care, bereavement coordinator, photographer — but the coordination load typically lands on the primary nurse, who is simultaneously managing a clinical case. The Resolve Through Sharing bereavement training (a two-day program with reported >95% participant comfort increase) exists precisely because most staff come into the unit without formal bereavement training, and the program fills that gap — but trained staff still need coordination scaffolding.
Research on multidisciplinary support after stillbirth and neonatal death identifies fathers as particularly likely to be overlooked in the coordination flow, because OB-centric staffing structures orient around the mother. Hospital-based programs like Mount Sinai's Perinatal Bereavement Support Program demonstrate that a dedicated program can coordinate across units, but the national picture remains uneven. The PLIDA bereavement coordinator job description outlines what a coordinated program requires, and the International Stillbirth Alliance coordinates standards globally — but local implementation is patchwork.
The family experiences this as inconsistent care. A couple who lost a baby in one unit at 2am and received a trained bereavement coordinator's presence within 45 minutes describes their care completely differently from a couple who lost a baby in the same unit at 2pm on a Saturday and never met the coordinator.
Solution Framework: A Shared Tapestry as Coordination Surface
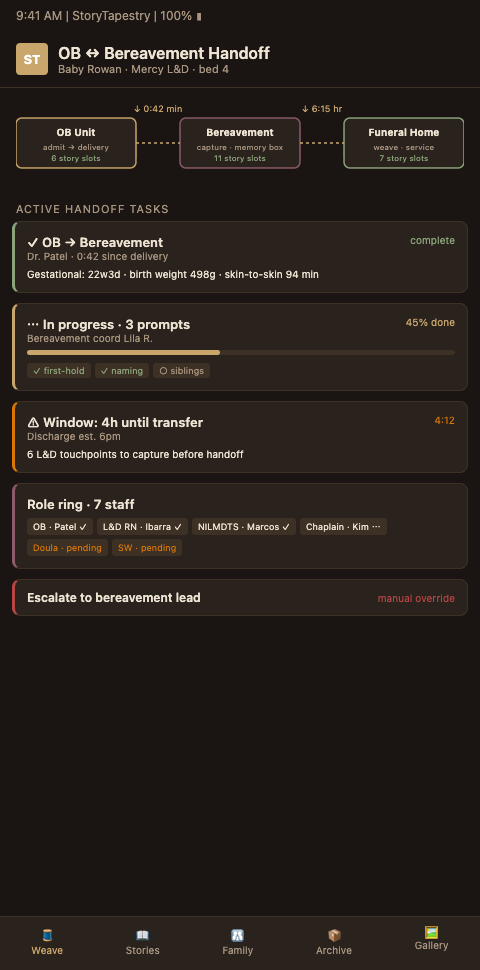
StoryTapestry treats cross-unit coordination as a shared surface, not a relay. The hospital's L&D team, NICU team, bereavement coordinator, social worker, chaplain, and photographer all write to the same tapestry with role-scoped permissions. Information does not have to be repeated. Decisions are visible. The family's experience is continuous even when the staff rotation is not.
The unit-agnostic record comes first. When a loss or impending loss is identified on any unit, a unit-agnostic StoryTapestry record is opened and assigned a coordinator. The record holds the clinical context (appropriately scoped), family preferences captured at intake, consent status for photography and memorial materials, and a thread list. Any team member entering the room can see at a glance: baby has a name yes/no, family has been offered memory box yes/no, photographer has been called yes/no, chaplain has been paged yes/no, sibling in the waiting room yes/no. The alternative — each unit keeping its own note — produces exactly the fragmentation the ScienceDirect review identifies.
Role-scoped participation. An L&D nurse can add clinical medical milestone records, a bereavement coordinator can add family-facing narrative content, a chaplain can add blessing and ritual notes, a photographer can upload captures. Each role sees the fields they can write and the fields they can read. A photographer does not need the clinical timeline; a clinical nurse does not need the photograph gallery. But all roles can see the family preferences layer, which is the cross-cutting context everyone needs.
Escalation paths encoded in the workflow. When a loss event is logged on L&D at 2am, StoryTapestry auto-pages the on-call bereavement coordinator, the on-call chaplain (if the family has opted in), and the photography volunteer pool. The paging is instrumented — response times are logged, and a weekly quality review shows which shifts have coverage gaps. This eliminates the dependence on a specific nurse remembering to page a specific person, which the Springer chapter identifies as the single most common coordination failure.
Family-facing unification. The family sees one coordinator and one tapestry. Internally, five or six staff may have contributed; externally, the family experiences a coherent presence. The coordinator is the named relationship, and the tapestry is the shared artifact. This mirrors the pattern in hospice coordination handoffs from adjacent bereavement domains, where a single named coordinator shields the family from the coordination complexity underneath.
Handoff preparation built in. The tapestry's structure already anticipates the hospital funeral handoffs step. When the family is ready to engage a funeral home, the handoff packet generates from the tapestry state automatically — the narrative summary, the family preferences, the thread inventory, the consent log. The coordinator reviews and releases rather than assembles. This turns a one-hour handoff prep into a 15-minute review.
Advanced Tactics for Unit Coordination Programs
Four tactics strengthen cross-unit coordination beyond a shared record.
First, run structured joint case reviews. Once a month, the bereavement coordinator, the L&D nurse manager, the NICU nurse manager, the chaplaincy lead, and the social worker meet for 60 minutes and walk through three recent cases. The tapestry is the agenda — threads each team member contributed, gaps that appeared, family feedback received. These reviews surface systemic patterns (e.g., the 11pm-7am shift consistently misses the photography call) that no individual unit would notice. The Mount Sinai program model anchors on joint case review as a coordination practice.
Second, cross-train staff across units. An L&D nurse who has spent a shift shadowing the NICU bereavement response becomes a better cross-unit communicator. The Resolve Through Sharing training fills baseline knowledge; unit-shadow rotations fill context. Budget quarterly cross-shadowing time and protect it from cancellation.
Third, appoint a dedicated perinatal bereavement coordinator. The PLIDA job description lays out the role: a 0.5-1.0 FTE position that coordinates the program, manages the tapestry system, trains new staff, and serves as the family's named relationship. Programs with a dedicated coordinator consistently outperform programs where bereavement coordination is distributed across clinical roles. If a full FTE is infeasible, start with 0.5 and grow.
Fourth, measure cross-unit handoff quality. Metrics: time from loss event to bereavement coordinator arrival at the bedside (target <60 minutes, ideally <30), percentage of cases with photography offered, percentage with chaplaincy offered (for families who opted in), percentage with both parents acknowledged (not just the mother), percentage with sibling offered participation if applicable. Review these monthly. Programs that do not measure these metrics plateau at adequate; programs that measure them improve steadily.
Fifth, fold bereavement coordination into unit onboarding. A new L&D nurse should meet the bereavement coordinator in week one, shadow a memory-box preparation in week two, and review the coordination workflow in orientation material. Making bereavement central to unit identity — rather than a rare specialty — changes how staff respond when a loss happens on their shift.
CTA: For OB and L&D Leadership Standardizing Bereavement Coordination
Your unit is delivering great bereavement care on some shifts and uneven care on others, and the gap depends more on which staff are working than on your stated protocol. StoryTapestry gives your program a shared coordination surface, role-scoped permissions, and automated escalation paging so quality does not rest on individual memory. Invite your bereavement coordinator, L&D nurse manager, chaplaincy lead, and social work lead to a 75-minute workshop. We'll map your current handoff points, identify the gaps the tapestry fills, and draft a joint case-review cadence tailored to your unit's volume. The workshop covers the four-role coordination surface, the role-scoped permission matrix, automated escalation paging tuned to your shift patterns, and a sample tapestry showing how the coordination surface tracks across a 36-hour bereavement event.
Pilot engagements include platform access for your bereavement coordinator, charge nurse lead, social work lead, and chaplain, plus a named implementation lead who supports the first 10 cases and facilitates the first two monthly case-review meetings. Most programs onboard their first case inside three weeks of contract signing and reach protocol-level coverage across all shifts by month four. Bring your L&D medical director, nurse manager, bereavement coordinator, chaplaincy lead, and social work lead — the workshop produces a unit-ready coordination protocol the full team can present to hospital leadership before the pilot starts.